
A deeper understanding of the anatomical form leads to an insight that has practical significance. This deeper understanding requires a way of looking. A way of looking that leads to seeing which turns illustrations of structures into living pictures of anatomy. The way of looking represents a state of mind. This state of mind is often biased by the rhetoric we use in order to describe what we are looking at. Being unaware of it, this rhetoric is often not without consequences for our daily practice!

RHETORICS OF ANATOMY
We all know the following description: the spinal nerve runs through the intervertebral foramen. Just as well we all know the descriptions: the Nervus vagus passes through the Foramen jugulare and the nervi olfactorii penetrate the base of the skull in order to make a synaps with the olfactori bulbus. When we look more closely at his kind of description, we can notice that it leads us to the assumption that the chronology of appearance is: first the bony structure and afterwards the nerve. However, just look at the rhetoric: if you run through something it can only be possible when that specific tunnel structure (Foramen) is already present. It is even more obvious when we use the description “penetrate”. This raises questions as for instance: how does the nerve do that – does it have a special drilling machine? Even more, how does the nerve know that it should do this – is there something like a sign: “drill here”?
RHETORICS AND PRACTICAL CONSEQUENCES
A couple of weeks ago I saw a lady and her new born in my practice. The girl was born premature (caesarean section at week 33) because the mother was diagnosed with pregnancy poisoning. The child is 8 months old now. About two months ago the mother noticed that her girl does not follow her optically as it should be at that age. After visiting the paediatrician and going through a series of test the verdict was quite harsh: the girl is turning blind! Already the optic function seems to be limited and it will most likely decrease. The following statement gave the reason for this problem: the Canalis opticus is too narrow for the optic nerve to run through. The parents are devastated by the verdict: the problem was found but there exists no solution for it. It was the grandmother who contacted me. If I could do something? Well, for an osteopath this is not something on the daily menu so I do not know, but let us give it a try.
Let us give it a try. NO, I was not looking for a specific technique that I could use on the optic system. Neither was I looking for a technical approach for the Ala minor of the sphenoid bone! I did not go through the book of Sutherland or Magoun looking for some cranial techniques. NO, I was going through my mind asking myself some questions. To begin with: does the nerve have a drilling machine to force its way through the narrow optic canal? Well, it doesn’t!! It does not because the anatomical description is rhetorically incorrect: neither does the optic nerve penetrate through the sphenoid bone nor does it runs through the optic canal.
To understand this you need to know and respect “chronology”!! So before I am looking immediately for some hands-on solutions, I am first and for all going through some (logical) steps of reasoning. And this requires items to reason from as well as correct rhetoric to start with. Needless to say that the items for an osteopath exist of the anatomical knowledge – dixit A.T. Still.
HOW DO NERVES KNOW THEIR WAY?
To assume that nerves know their way requires the assumption that nerves have the capability “to know”. As far as my knowledge reaches: nerves do not posses the necessary structures to be able “to know” – simply stated: nerves do not have brains! And no, I am not satisfied with the “scientific assumption” that somewhere in the DNA of the nerve some path-following-drilling-instructions are encrypted!! So the assumption/conclusion that nerves know their way is based upon the wrong premises – simply stated: nerves do not know their way. So how come that nerves are always found in certain areas of the body? Moreover, it looks as nerves always follow a certain trajectory that leads them into a certain part of the body. How do they do it?
Looking into anatomical details, we cannot deny that there is a principle: nerves are always accompanied by blood vessels. This is certainly quite obvious in the macro-anatomical dimension – for instance: femoral artery, vein and nerve. And when we look more closely into smaller dimensions, we observe the same positional relationship. Question: if we see this in all dimensions, where does this relationship come from? To understand it we have to look more closely into the development of these different structures.
Principle: nerves are accompanied by blood vessels. Again a rhetorical error – even the spelling correction on the computer gives this us this proposal!! Nevertheless it is a rhetorical error because it should be formulated: blood vessels are accompanied by nerves. And this for a very simple reason. When we study the development of the nervous system we cannot deny the fact that nerves only appear in those regions where prior to the growth of nerve extensions, we first observe signs of blood vessel existence! With other words, in respect to the chronology of appearance/existence: blood vessels come before nerves! With other words: absence of a blood vessel leads to absence of a nerve; not vice versa!
But wait a minute!! Remark: this is not always the case!! In the case of very small nerve endings, blood vessels do not necessarily exist … . Well, I am sorry to say so but the principle still stands because even in those regions we have “a kind of blood vessel behaviour”. How so? Let us look into the mechanism behind blood vessel development.
Blood vessel development requires a number of conditions. These are: existence of fluid, cells, a trajectory (= current as a consequence of concentration gradient) and cyst development. Fusion of these cysts leads to the formation of primary blood vessels, a phenomenon called angiogenesis. But before we can observe this structuration on cellular level, we have to emphasize that blood vessel development is characterized by the primordial existence of a current representing a fluid trajectory. Which means a current with a main direction in which these cysts appear. With other words: if there is no current in form of a trajectory there will be no blood vessel development.
We have just seen that we can notice a specific chronology when it comes to the appearance of nerves and blood vessels. Yes, these structures have an intimate relationship. But where does this come from? Yes, we have seen that blood vessels appear before nerves. Does this mean that nerves follow blood vessels? Is this the relationship? No, it is the fact that a blood vessel and nerve share the same developmental condition: a fluid trajectory! So there you have it: even where nerves do not accompany blood vessels (for instance in the case of very small nerve endings), these nerves are taken along by the existing current that is one of the basic conditions for blood vessel development! So nerves know their way by simply being guided by a current!! (for dendrites and axons this guidance is slightly different but the principle is nevertheless the same)
RESTRAING INFLUENCE
Once when blood vessels are developed under these specific conditions (see above) we can notice that the speed of growth is increasing. We could say: blood vessels support and even increase the speed of development – because less information is lost on the way to the periphery. Plain and simple? No, there is more to it. There is more to it because we can observe that, together with the structuration of the current, the blood vessel itself starts to resist that growth. Not by slowing down the speed of growth, it is much more “giving growth a specific direction – “the way of less resistance”. Observing this phenomenon of growth direction (developmental pattern) we come to the conclusion that blood vessels are a paradox: they increase growth and at the same time they behave restraining.
Blood vessels are the first real (anatomical) structures we can observe in the developmental process. Blood vessels are therefore the first restraining structures. But they are not the only ones! To understand this we have to keep in mind that the blood vessels (just as all future restraining structures) are derivatives of a specific origin called inner tissue.
INNER TISSUE
ABOUT TERMS
Most colleagues are familiar with terms such as mesoderm and connective tissue. These two terms could/should be seen as synonyms of each other. However, there is a catch to it! In the case of mesoderm the emphasis lies on the cellular component, which means that the presence of water and matrix as basic components is simply ignored. In the case of connective tissue, we all know that this tissue is characterized by the presence of water, matrix, cells and fibres. However, although we know this, many of our colleagues, certainly today, are too focussed on the fibre component. Again water and matrix are ignored (cells less). And do not forget, if mesoderm and connective tissue are synonyms, mesoderm does not contain fibres – certainly not in the beginning. So for both terms, mesoderm as well as connective tissue, we have to look at and respect chronology in order to understand the full meaning of them!!
Before we end up in a Babylonian confusion, we can simply unite mesoderm and connective tissue (as almost being synonyms) by using another term: inner tissue. The term “inner” comes from the fact that it is representing that part of space that is incorporated within our body. More over, containing water-matrix-cells-fibres (in this chronology please), the inner tissue is the source for all metabolic activity (so growth and development as well)! Moreover, as development proceeds we can observe that this inner tissue changes its way of appearance. It becomes more and more structured – see for instance blood vessels as being a derivative of the inner tissue. And as structuration of the inner tissue becomes more and more evident, this inner tissue behaves more and more restraining. We can conclude this due to the fact that, with the appearance of a more structured inner tissue, the growth of organs as well as the growth of the organism as a whole shows more and more directional characteristics.
MANY DIFFERENT WAYS OF APPEARANCE
Inner tissue has many different ways of appearance; it can be a very liquid form (such as for instance blood) or a very dense form (such as for instance bone). In between these two extremes there exists a wide variety depending on the ratio between the different components. When we look at the chronological appearance of the 4 components water-matrix-cells-fibres we can observe that when we shift more and more to the right, then permeability (metabolism, growth) decreases and density (restrain) increases. And of course vice versa. In this context we can classify anatomical structures for instance as follows: fluids – blood vessels – fascias – bones. Please keep in mind that ligaments as well as tendons are merely parts of fascia depending on the amount of fibres and the direction within that fascia.
When we look now at the different forms of this inner tissue we can observe a very interesting characteristic. This is the fact that within the inner tissue space these anatomical structures, originating from one or more components of the inner tissue, and although they have a different texture, these structures have one thing in common: they have the same spatial orientation. This means that within these structures we can observe the same trajectorial features! In order to understand this, please compare for instance the fibre direction of the Falx cerebri and Tentorium with the fluid trajectory of the dural sinuses. Or look more closely to the anatomical features of the muscles and fascias of the skull and trunk and you can see the continuity of pattern!
The question that rises now is: how can the inner tissue eventually have so many different ways of appearance?
To begin with we can ask ourselves: what is development? The moment of fertilisation is the starting point of a so-called change of the original balance for the cell. This results into a phenomenon that represents a constant search for a (new) balance. It is called metabolism. Whenever this metabolism cannot maintain or does not lead to a new balance, the initial dysbalance leads into a change of the original form by cleavage or apoptosis. This cleavage, a phenomenon expressing a continuous search for balance, leads to growth. Development is merely an expression of that growth but with a distinct difference: development = growth with specific direction = growth with a restraining influence => a part of the inner tissue cannot follow growth with the same speed of change.
Following this line of thought we can make the following conclusion:
A change of texture (density/permeability) of the inner tissue is a consequence of the interaction between metabolism/growth (expansion) of an organ and the surrounding components of the inner tissue. As soon as one or more of these components of the inner tissue cannot follow the event of metabolism/growth, this or these components of the inner tissue behave as restraining apparatuses. The more we have a restraining influence the more we will have an impact on the form and function (metabolism/growth) of the organ/organism. The impact will be directional (trajectorial).
RELATIONSHIP WITH NERVES
Nerves, derivatives of the ectodermal layer, should be seen as organs. Like all organs, nerves are also functionally related to the inner tissue. In the case of nerves there is however a specific characteristic: nerves are completely surrounded by inner tissue. So nerves are embedded within the inner tissue space. And this has consequences!
Development, growth with direction, is characterized by different phenomena.
The first phenomenon is the fact that growth equals expansion. This is why development is also called expansion growth. Expansion means that not only the size of the form (external features) but also the size of the inner tissue space (internal features) is increasing!
Another phenomenon is the fact that the space involved in the development becomes transformed. This transformation is mainly a consequence of restraining influences. Development therefore is characterized by specific growth directions induced by restraining influences of one or more components of the inner tissue.
Previously we have seen that the development of blood vessels appears prior to the development of nerves. Both have one thing in common: a current. This current is nothing more than simply changing the form of the fluid according to the direction of less resistance! And as the current become more structured, it behaves more and more restraining – more trajectorial. Interesting to see is the fact that this causes no conflict as such for our nerves! There is no conflict because the nerve runs parallel to the direction of the restraining influence. Moreover, the nerve is already present long before the inner tissue changes into a more dense structure (chronology: fluid – blood vessel – fascia – bone).
With other words: the nerve does not go through a Foramen intervertebrale nor does it penetrate a Lamina cribrosa of the ethmoid bone. Instead the inner tissue derivatives such as blood vessel, fasciae, cartilage and bone develop around the nerve. Moreover, these structures develop according to the same growth directions as the nerves do!
So where does the conflict come from causing the girl’s nerve to get into distress in such a way that the optic function becomes endangered?!
TANGENTIAL & PERPENDICULAR PATTERN
PRINCIPLE
Looking into the anatomical details of the optic system we have to study the different structures of the inner tissue as they appear in different densities (fluid – blood vessel – fascia – bone). Doing so we can observe that they represent two types of spatial orientations: longitudinal and transversal to the trajectory of the optic nerve. In fact, if we want to be complete and correct we have to add a third one that is called spiral-diagonal, which is in fact a combination of the first two.
Whenever the patient’s body is put under stress, these inner tissue derivatives will “guide” that stress into the “way of ease. This can be observed by palpation as a physical stress pattern. It is unnecessary to say that the direction of these pattern correspond with the original growth directions initiated by the restraining influence of the inner tissue! For this reason these stress directions can be called developmental or (as I prefer to call them) morphokinetic pattern – present even after birth.
Another phenomenon that we can observe in practice is the fact that these two patterns do not have the same impact for the form & function of nerves. Concrete: as long as a pattern “runs along” the trajectory of the nerve (parallel), the impact on the metabolism seems to be minor (less clinical signs). In the case that such a pattern “crosses” (perpendicular) the trajectory of a nerve, the impact seems to be stronger (more clinical signs). One of the explanations for this phenomenon is the fact that in the case of crossing patterns the axoplasmatic transport (a current!) is disturbed. And this for sure has an impact on the nerve function as EMG studies have proven!

Illustration 1:
As a scheme some of the different developmental patterns of the neurocranium and viscerocranium are indicated by arrows. The scheme shows the different anatomical relationships as a basis for practice. (JP.Höppner - seminar "Anatomy & Ontogenesis", Madrid 2019)
NEUROCRANIAL PATTERN
Neurocranial patterns are stress directions within the anatomical neurocranium. The neurocranium consists of derivatives of the inner tissue that are surrounding the brain, brainstem, spinal cord and all of the spinal and cranial nerves. The neurocranial patterns can express the restraining influence of the various derivatives of the inner tissue. Therefore such a restraining structure, causing a certain pattern, can be a fluid, a blood vessel, a fibrous structure such as the Dura mater and finally even bone (trabeculae!).
Related to the form & (dys)function of the optic system we are now looking for restraining structures, not so much parallel but more perpendicular to the trajectory of this optic system.
One of the first structures that pops-up in the anatomical mind is the restraining apparatus known as the dura girdle. There are 3 of these girdles: anterior, medial and posterior. These girdles develop as restraining structures during brain development. We have to keep in mind that these girdles, although subdivided into three individual parts, in reality are one and the same continuous fibre system. The only feature that is different is the fact that they have different spatial orientations. Looking at this individual spatial orientation it becomes clear that only the medial girdle represents a stress pattern that is standing perpendicular to the trajectory of the optic system.
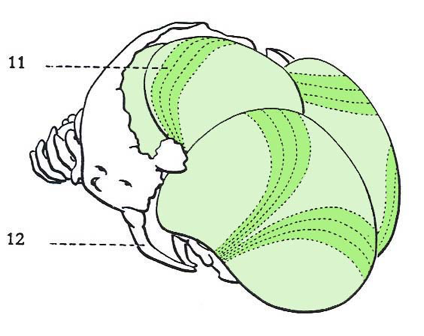
Illustration 2:
Lateral-superior view on the skull localising the posterior and medial dura girdle. Please notice that the medial dura girdle is situated in the region of the future coronal suture as well as the parietal and metopic suture. The darker green color simply indicates the higher concentration of fibres in the Pachymeninx that surrounds the future brain.

Illustration 3:
Please notice how the fibres of the three girdles are crossing in the region of the base of the cranium. Please also notice the fact that the medial girdle crosses the optic nerve and tract perpendicular. (both illustrations - Blechschmidt, Karger Basel 1960, page 257)
For those who are not acquainted with this structure, keep in mind that this dura girdle is situated parallel to the orientation of the coronal suture extending fan-like from the base of the cranium towards the anterior fontanel (bregma).
It is interesting to see that in the case of the little girl there is a distinct clinical sign in the region of the skull. On the level of the coronal suture there is a distinct depression. A depression that can also be observed in the region of bregma. In both cases it is a clear indication for a restraining influential pattern caused by the medial dura girdle! Putting these fibres under stress means a densification of the inner tissue and consequently an impact not only on the calvaria but also on the base of the cranium in the region of the optic canal (know your anatomy !!).
Since the inner tissue leads to many different derivatives (with a same direction) we can ask ourselves if it could also be a vascular structure that causes a pattern disturbing the region of the optic system. Well of course it can be. Simply use the same pattern and fill it in by the dural sinuses such as the Sinus sphenoparietalis and its continuity to the other venous structures. Or study the vascularisation of the brain itself. And if you want a bony pattern simply visualise the trabecular system of the future bone structures. Once again, know your anatomy: macro- and micro-anatomically.
But in the case of this girl it was definitely related to the dura girdle. Palpation clearly showed that, due to the texture of the pattern, there is no doubt. After all, a pattern is a physical event that has a specific texture related to the restraining structure (fluid = viscosity, cell = turgor, fibre = tension, all together = malleability). In the case of the girl the pattern showed all palpatory features of tension indicating a stress within the fibre component of the inner tissue.
The child was born October 2018, which means almost 8 months ago at he moment when I see her for the first time. This means: no time to waste!! Because, as we all know, the anterior fontanel “closes” by the 12 month. And once it is closed, the possibilities of influencing this region become more and more difficult (the more density there is, the more resistance it will give – also against a treatment!). However, of course the anterior fontanel does not close by the 12 month! Would this be the case we would have a major problem for further brain development. In fact, we still have time till the age of 6 years. But unnecessary to say, that with time passing by, the pattern becomes more and more a part of the form and consequently more and more difficult to treat.
VISCEROCRANIAL RELATED
When we study the human development we can observe that the growth of the brain (process of cerebralisation) is characterized by specific patterns. These patterns are a consequence of restraining influence coming from different structures of inner tissue origin. Different specific directions characterize such patterns. Looking at the form of an anatomical structure we can identify these patterns by the positional relationships of its components (form is the consequence of its structures and their positional relationships, relationships which result from developmental pattern). Adding all these directions together we can observe in relationship to the brain a trajectorial vector called “ascensus” (blue arrow in illustration 4).
In the same way we can observe in relationship to the viscerocranium a so-called descending pattern (red arrow in illustration 4). But keep in mind: viscerocranium means more than just the region of the face! It also includes the neck and trunk region !! With other words, we have to extend the anatomical relationship within the region of the face into the region of the trunk.
The so-called pattern of the viscerocranium is called “desensus”. A central key role in this developmental event is the repositioning of the future Centrum tendineum (phrenic part) of the abdominal diaphragm. This pattern is quite complex. Too complex to describe here in detail but what we need to know in the case of this girl, is the fact that many of the forces caused by this pattern are focused towards the base of the cranium. The descending forces cause a change of the face as for instance it repositions the palatum durum and molle and influences the sphenoid bone (formation of pterygoid process) (see illustration 1: red arrows in the region of the gut entrance).
Why is this process of repositioning so interesting in the case of the child? Isn’t the problem a neurological one? What has the eye to do with the abdominal diaphragm? It is interesting to notice that the child, during the time of breastfeeding, repeatedly gave back some of the milk and had hick up afterwards. The hick up even persists today. Moreover, it can be noticed that the girl is sucking on her left thumb… . Looking more closely at the child (palpation chest) it can be observed that breading does not happen symmetrically. Moreover, there is a slight side bending of the child to the left. The latter is a clinical sign for which it receives physical therapy (exercises to train the muscle chains in order to become symmetrical).
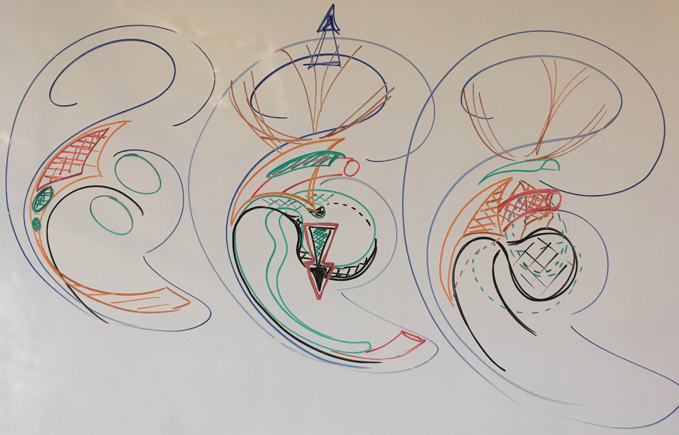
Illustration 4:
The illustration shows the impact of the centrum tendineum (in black) which is also called septum transversum or pars phrenicum of the future abdominal diaphragm. The septum arises in the cervical region and will become repositioned during development. A complex movement that changes the complete form of the trunk (chest development - see orange color, extending also towards the pelvic region!). This developmental movement also has an impact on the development of the face (compare medial illustration with the first picture shown previously in this article). (JP. Höppner - seminar Anatomy & Ontogenesis, La Bresse 2019)
So yes it is interesting to notice these clinical signs because they are embedded in a viscerocranial pattern. And keep in mind that these signs are caused by a pattern that focuses on the anterior part of the base of the cartilage skull as well. And do not forget: this skull has not yet completely densified into a real bone structure. Can it be that, besides the pattern of the dura girdle, this “visceral” pattern also contributes to a “neuronal” developmental process that maybe is preceding a bit too fast? A bit too fast causing stress for the optic nerve by squeezing it?
STUDYING THEORY = DOING PRACTICE
Most of the things I have described in the text above went through my mind before I saw the girl. Even more mental constructions came up before I did put my hands on her. Finally, the palpation was nothing more and nothing less than a confirmation/deconfirmation of the large number of possibilities there are to be uncovered. In fact the complete treatment was a process of several steps, one following after the other.
The first step in the process was: questioning the definition of the problem. NO, nerves do not go through, pass or penetrate. Nerves do not have a drilling machine to clear their way. Nerves, in form & function, are a consequence of environmental circumstances located within the inner tissue space. And it all starts with the presence of a current. A current that outlines a specific direction in form of a pattern for future anatomical structures.
The next step was identifying which pattern influences the function of the optic system. This means that first one needs to know his/her anatomy so he/she can build a living picture of anatomy in his/her mind. If this picture does not exist, you can look but will not see. As it happens so often: looking at a picture does not mean that you know the meaning of it, it requires more than just looking in order to understand!
And yes, it all starts with a fluid but this does not mean that by simply/only working in or with the fluid the problem will be solved automatically! Restraining influences do come from different trajectorial structures!! So, not only do we need to know our anatomy, we also need to know what textures that they have. Because in the process of identifying the pattern the second part is focussed on the palpatory information in order to confirm/deconfirm the mental construction. Identifying the texture of the pattern is a crucial palpatory contribution to the process of pattern visualisation. (Something your learn quite well by doing anatomical dissections, unfortunately not by merely studying books!)
And once the pattern is identified it becomes obvious what to do: either we go along, either we go in the opposite direction of the trajectory. In both cases there is only one intention: getting the stress out of the restraining structure. Beside the fact that you have to be very accurate – the technique as such is simple.
And finally: after finding – fixing – leaving, we wait and see what nature will do with it.
In the case of this girl we are dealing with a pattern in the complexity level of fibres. This means that nature approximately needs up to 9 months to reconfigure the spatial organisation (process of internal reorganisation). It is not a good idea to wait that long before making a new appointment. Certainly not in this case because humans of that age are little monsters and they have their own time scale! In general it goes faster than in adults and unfortunately this takes place in both ways. So time is of the essence in our treatment.
What the outcome finally will be? No idea, we will see – as a figure of speech. But at least I tried. I tried by reasoning. Reasoning that is based upon the profound knowledge of anatomy. Just as A.T. Still wants us to do it. That is one of the things I learned from studying his literature.
